Erector Spinae Plane Block (ESPB)
The erector spinae plane block deposits local anaesthetic into the fascial plane between the erector spinae muscle group and the transverse processes of the vertebrae. The erector spinae muscles (iliocostalis, longissimus, spinalis) lie posterior to the transverse processes. Local anaesthetic spreads both cranially and caudally, and can track anteriorly around the transverse processes to reach the ventral rami, dorsal rami, and potentially the paravertebral space and epidural space. The block provides both somatic and visceral analgesia.
Indications
- Multiple rib fractures and thoracic wall trauma
- Post-thoracotomy pain (posterolateral approach)
- Upper abdominal surgery analgesia (hepatobiliary, oesophageal)
- Laparoscopic cholecystectomy
- Spinal surgery supplemental analgesia
- Hip fracture (lumbar ESPB)
- Total hip arthroplasty
- Neuropathic pain (herpes zoster, post-herpetic neuralgia)
- Chronic thoracic/lumbar pain
- Mastectomy and breast reconstruction
Contraindications
- Patient refusal
- Active infection or skin breach at injection site
- Significant coagulopathy (risk-benefit assessment required)
- Known allergy to local anaesthetic agents
- Severe anatomical distortion (e.g., significant scoliosis)
- Inability to maintain position for procedure
Technique
- Patient positioned prone, sitting, or lateral decubitus
- High-frequency or curvilinear probe (depending on depth) placed in parasagittal plane, 3 cm lateral to midline
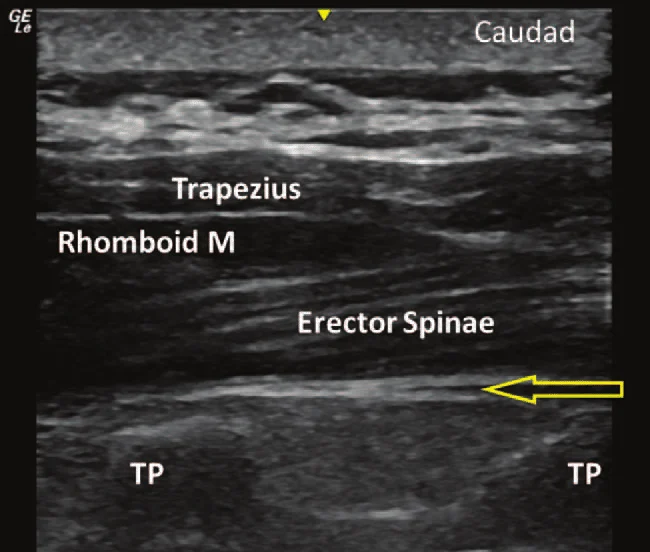
- Identify transverse process (hyperechoic shadow with acoustic shadow), overlying erector spinae muscle, and trapezius/rhomboid superficially
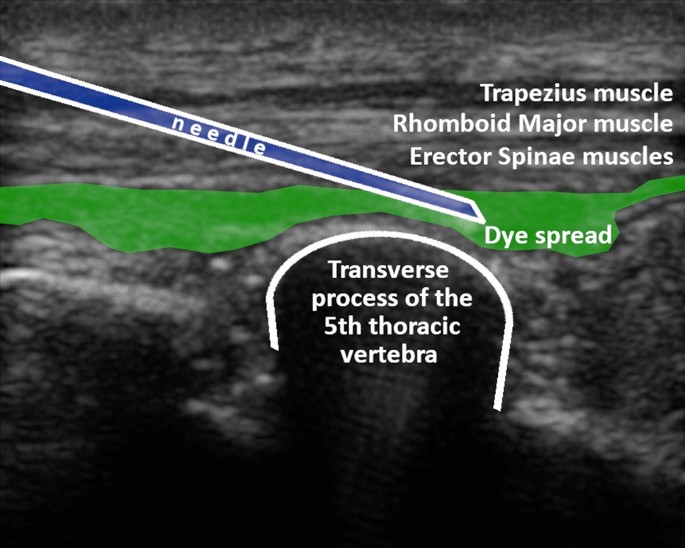
- Target the plane deep to erector spinae and superficial to transverse process tip
- In-plane needle insertion from caudal to cranial direction
- Needle tip confirmed at transverse process; hydrodissection with 1–2 mL saline
- Inject 20–30 mL local anaesthetic; confirm spread lifting erector spinae muscle off transverse processes
- Catheter insertion possible for continuous infusion
Drug Doses
| Agent | Concentration | Volume | Total Dose | Notes |
|---|---|---|---|---|
| Ropivacaine | 0.375–0.5% | 20–30 mL per side | 75–150 mg | Preferred for ESPB; good sensory block with minimal motor blockade. Max 3 mg/kg. |
| Levobupivacaine | 0.25% | 20–30 mL | 50–75 mg | Long-acting, less cardiotoxic than bupivacaine. Excellent for prolonged analgesia. |
| Bupivacaine | 0.25% | 20–30 mL | 50–75 mg | Max 2 mg/kg. Use with caution in bilateral blocks due to cumulative dose. |
| Bilateral ESPB | 0.25% ropivacaine | 15–20 mL each side | Calculate cumulative: ≤3 mg/kg ropivacaine total | Bilateral blocks require strict dose calculation. Consider diluting to 0.2% for bilateral use. |
Complications
Landmarks
- Spinous processes (midline landmark)
- Transverse processes — target structure; typically 3–5 cm lateral to midline
- Erector spinae muscle group (lying superficial to transverse processes)
- For thoracic ESPB: T5 transverse process recommended for mid-thoracic coverage
- For lumbar ESPB: L3–L4 transverse process for lower abdominal/hip coverage
Sensory Coverage
Somatic: ipsilateral posterior and lateral chest/abdominal wall over multiple dermatomal levels (typically 4–6 levels caudal to injection). Visceral component via paravertebral/epidural spread is variable. Bilateral blocks provide circumferential thoracic/abdominal coverage.
Clinical Pearls
Background & Evidence
First described by Forero et al. in 2016, the ESPB has rapidly gained popularity as a versatile truncal block. Its relative distance from the neuraxis and pleura makes it safer than paravertebral and epidural blocks, with a broader learning curve. It provides both somatic and potentially visceral analgesia, though the visceral component is variable and less reliable than true paravertebral blockade. Cadaveric studies show spread to the paravertebral space and epidural space occurs in a proportion of cases.
Ultrasound Images