Serratus Anterior Plane Block (SAPB)
The serratus anterior plane block (SAPB) targets the intercostal nerves (T2–T9) within the fascial plane superficial or deep to the serratus anterior muscle. The serratus anterior originates from the anterior surfaces of ribs 1–9 and inserts onto the medial border of the scapula. The lateral cutaneous branches of the intercostal nerves pierce the intercostal muscles and pass through or superficial to the serratus anterior muscle to supply the lateral chest wall.
Indications
- Rib fractures (multiple rib fractures — excellent analgesia)
- Post-thoracotomy pain (lateral thoracotomy approach)
- Breast surgery analgesia (mastectomy, wide local excision)
- Chest drain insertion analgesia
- Thoracoscopic procedure analgesia
- Lateral thoracic wall trauma
- Axillary surgery
- Post-thoracostomy pain management in ICU
- Herpes zoster (acute/chronic neuropathic pain)
Contraindications
- Patient refusal or inability to cooperate
- Infection or cellulitis at injection site
- Significant coagulopathy (INR >1.5, platelets <80, anticoagulant therapy — assess risk/benefit)
- Known allergy to local anaesthetic agents
- Overlying malignancy at injection site
- Distorted anatomy precluding safe identification of target structures
Technique
- Patient positioned supine or lateral decubitus with ipsilateral arm raised
- High-frequency (10–15 MHz) linear ultrasound probe placed in mid-axillary line at 4th/5th rib level
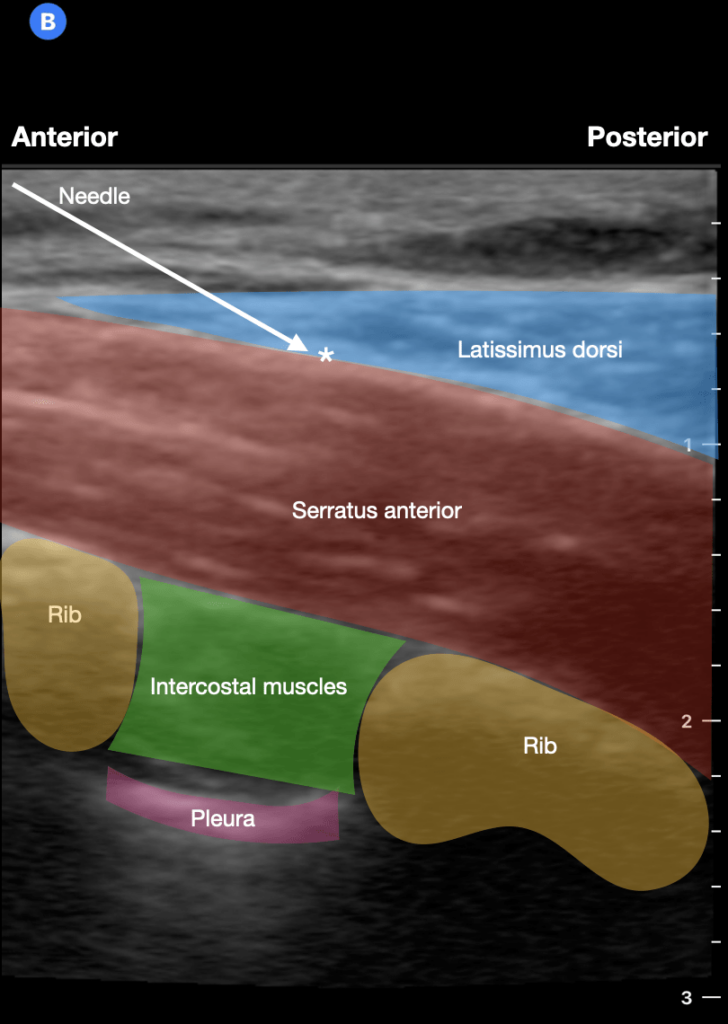
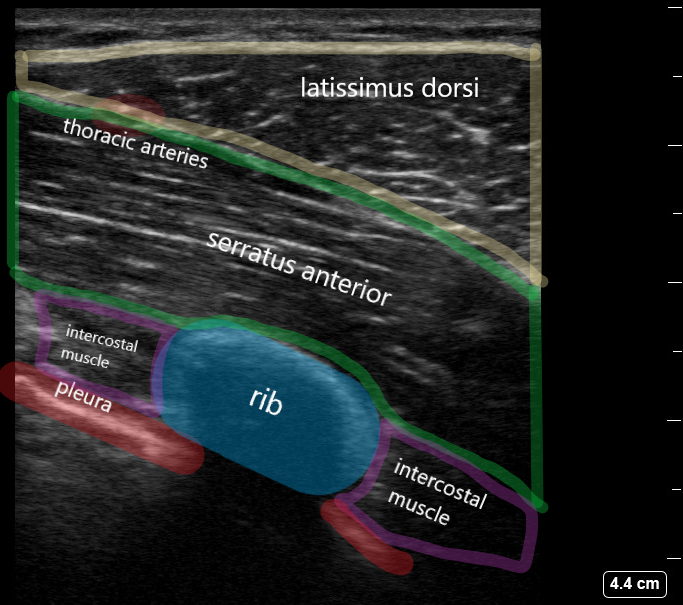
- Identify serratus anterior muscle (fan-shaped, sitting on rib surface) and overlying latissimus dorsi
- Two approaches: (1) Superficial — inject between latissimus dorsi and serratus anterior; (2) Deep — inject between serratus anterior and ribs (more reliable spread)
- In-plane needle technique recommended; advance to target fascial plane
- Hydrodissection with 1–2 mL normal saline to confirm correct plane
- Inject 20–30 mL local anaesthetic with regular aspiration every 5 mL
- Visualise spread within fascial plane on ultrasound
Drug Doses
| Agent | Concentration | Volume | Total Dose | Notes |
|---|---|---|---|---|
| Levobupivacaine | 0.25% | 20–30 mL | 50–75 mg | Preferred agent in EM; less cardiotoxic than racemic bupivacaine. Excellent for prolonged analgesia. |
| Ropivacaine | 0.375% | 20–30 mL | 75–112 mg | Good sensory/motor separation. Max dose 3 mg/kg. Excellent safety profile. |
| Bupivacaine | 0.25% | 20–30 mL | 50–75 mg | Max dose 2 mg/kg (NOT for IV use). Do not exceed 150 mg total. |
| Ropivacaine + Dexamethasone | 0.375% + 8 mg dexamethasone | 20–30 mL | 75–112 mg ropivacaine | Addition of dexamethasone may extend duration by 4–8 hours (perineural use off-label). |
Complications
Landmarks
- Middle axillary line at the level of the 4th or 5th rib
- Serratus anterior muscle (visible as serrated muscle fibers over the ribs)
- Latissimus dorsi muscle (posterior landmark)
- Rib surface as bony landmark on ultrasound
- Intercostal vessels — identify with colour Doppler to avoid
Sensory Coverage
Lateral chest wall T2–T9 dermatomes (mid-axillary line distribution). Does NOT cover posterior chest wall or parasternal region. Bilateral blocks are feasible.
Clinical Pearls
Background & Evidence
The SAPB was first described by Blanco et al. in 2013. It has become one of the most popular chest wall blocks in emergency medicine due to its relative safety, ease of learning, and efficacy for rib fracture analgesia. The RCEM position statement supports its use in emergency department settings by trained practitioners. Studies show significant reduction in opiate requirements, improved respiratory function (forced vital capacity, FVC), reduced pneumonia risk in rib fracture patients, and earlier mobilisation.
Ultrasound Images