Fascia Iliaca Compartment Block (FICB)
The fascia iliaca compartment block delivers local anaesthetic into the fascia iliaca compartment — a potential space beneath the fascia iliaca that contains the femoral nerve, lateral femoral cutaneous nerve (LFCN), and obturator nerve. The fascia iliaca is a thick fascial layer covering the iliacus and psoas muscles. The femoral nerve (L2–L4) lies lateral to the femoral vessels beneath the fascia iliaca and inguinal ligament. The LFCN (L2–L3) typically exits medial to the anterior superior iliac spine (ASIS). The obturator nerve runs deeper in the pelvis.
Indications
- Proximal femur fracture (neck of femur, intertrochanteric fracture) — first-line EM analgesia
- Femoral shaft fracture
- Hip dislocation
- Knee surgery / femoral condyle fractures
- Skin grafting from anterior thigh
- Femoral arterial line/catheter insertion analgesia
- Painful quadriceps haematoma
- Burns to anterior thigh
- Hip arthroplasty (post-operative analgesia)
- NICE guideline NG111 recommends fascia iliaca block for proximal femur fractures in the ED
Contraindications
- Patient refusal
- Infection at injection site (inguinal cellulitis, abscess)
- Significant coagulopathy — relative contraindication; risk vs benefit in NOF fracture (RCEM guidance: do not withhold for anticoagulant use alone if clinically indicated)
- Known allergy to local anaesthetic
- Previous femoral vascular surgery (distorted anatomy)
- Lymphoedema (increased infection risk)
- Inability to cooperate
Technique
- Patient supine; expose inguinal region
- LANDMARK METHOD (if ultrasound unavailable): palpate ASIS and pubic tubercle; divide inguinal ligament into thirds; injection point at junction of medial and lateral thirds; 2-click technique (fascia lata then fascia iliaca)
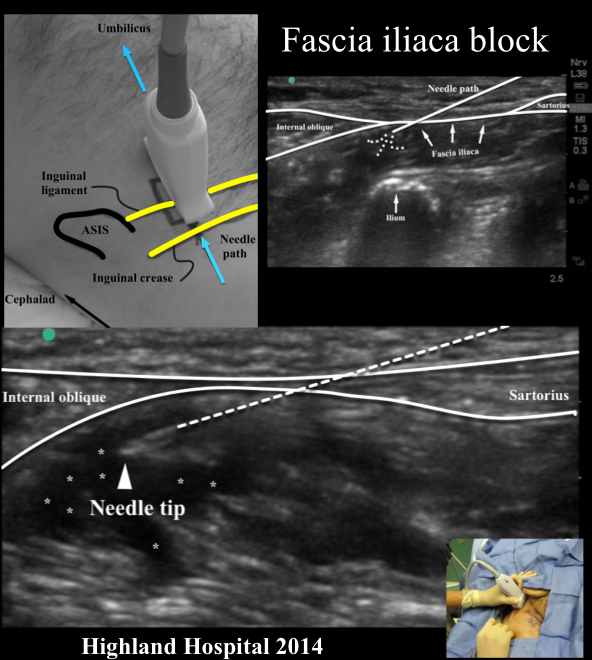
- ULTRASOUND METHOD (preferred): Linear probe placed infrainguinal, parallel to inguinal ligament, lateral to femoral artery
- Identify fascia iliaca (bright hyperechoic layer) overlying iliopsoas muscle
- In-plane needle from lateral to medial; target plane deep to fascia iliaca and superficial to iliopsoas
- Hydrodissect with 1–2 mL saline; confirm spread lifting fascia iliaca off iliopsoas
- Inject 30–40 mL local anaesthetic slowly with aspiration every 5 mL
- For superior FICB (Hebbard approach): probe placed more superiorly, medial to ASIS — higher obturator nerve block rate
Drug Doses
| Agent | Concentration | Volume | Total Dose | Notes |
|---|---|---|---|---|
| Levobupivacaine | 0.25% | 30–40 mL | 75–100 mg | Recommended by RCEM/BPS. Long duration 12–18h. Max dose 2 mg/kg. Most commonly used in UK EDs. |
| Ropivacaine | 0.375% | 30–40 mL | 112–150 mg | Good safety profile. Max 3 mg/kg. Comparable efficacy to levobupivacaine. |
| Bupivacaine | 0.25% | 30–40 mL | 75–100 mg | Max 2 mg/kg; do not exceed 150 mg. Higher cardiotoxicity risk than levobupivacaine — avoid in cardiac disease. |
| PAEDIATRIC (>5 years) | Levobupivacaine 0.25% or Ropivacaine 0.2% | 0.5–1 mL/kg (max 30 mL) | ≤2 mg/kg levobupivacaine; ≤3 mg/kg ropivacaine | Weight-based dosing essential in children. Lower concentrations reduce toxicity risk. |
Complications
Landmarks
- Anterior superior iliac spine (ASIS)
- Pubic tubercle (medial landmark)
- Inguinal ligament (line between ASIS and pubic tubercle)
- Femoral artery (medial to femoral nerve — to be avoided)
- Femoral nerve (lateral to artery, beneath fascia iliaca and fascia lata)
- Iliopsoas muscle (target muscle belly beneath fascia iliaca)
Sensory Coverage
Femoral nerve: anterior thigh and medial lower leg (saphenous nerve). Lateral femoral cutaneous nerve: lateral thigh (variable). Obturator nerve: medial thigh (variable — more reliable with superior approach). Does NOT cover posterior thigh (sciatic nerve territory).
Clinical Pearls
Background & Evidence
The fascia iliaca block is the most widely used regional technique in UK emergency departments, primarily for proximal femur fractures. NICE guidance (NG111, 2017) recommends it within 60 minutes of ED arrival. Studies show it reduces opioid requirements, delirium rates, and time to first mobilisation. The RCEM clinical standards recommend all EDs performing hip fracture care should have competent practitioners available to perform FICB. The superior approach (Hebbard technique) has demonstrated more reliable obturator nerve blockade in cadaveric and clinical studies.
Ultrasound Images